Printable Vaccine Consent Form
Printable Vaccine Consent Form - The eua is used when circumstances exist to justify the emergency use of drugs and. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. I consent to, or give consent for, the administration of the vaccine(s) marked above. (a) the patient and at least 18 years of age; I consent to receiving the seasonal influenza vaccine. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which was provided with this consent and release. Further, i hereby give my consent to walgreens or duane reade and the licensed healthcare professional administering the vaccine, as applicable (each an “applicable provider”), to. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. I consent to, or give consent for, the administration of the vaccine(s) marked. (b) the legal guardian of the patient; Except for the last two (2) questions, a “yes” response to any other question. I will stay in the pharmacy for at least 15 minutes after the injection and seek medical attention if needed. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. Please provide a copy of this form to your physician and/or healthcare provider for your permanent medical records. I consent to receiving the seasonal influenza vaccine. Except for the last two (2) questions, a “yes” response to any other question. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when administered by a primary care provider. (i) the patient and at least 18 years of age; (b) the legal guardian of the patient; (a) the patient and at least 18 years of age; I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which was provided with this consent and release. Tell your vaccination provider about. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which was provided with this consent and release. (b) the legal. I consent to, or give consent for, the administration of the vaccine(s) marked. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. I consent to receiving the seasonal influenza vaccine. I understand the benefits and risks of the vaccine(s). I. In addition, i am aware that the personal health information. (a) the patient and at least 18 years of age; By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. (b) the legal guardian of the patient; I consent to, or. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. Or (ii) the patient’s personal representative. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when administered by a primary care provider. (a) the patient and at least 18 years of. Please provide a copy of this form to your physician and/or healthcare provider for your permanent medical records. I consent to, or give consent for, the administration of the vaccine(s) marked above. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted. (a) the patient and at least 18 years of age; Except for the last two (2) questions, a “yes” response to any other question. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when administered by a primary care provider. I consent to, or give consent for, the. I hereby consent to the administration of the flu vaccine for which i have signed below be given to me or the person named above for whom i am authorized pursuant to sections 431.058,. (b) the legal guardian of the patient; I will stay in the pharmacy for at least 15 minutes after the injection and seek medical attention if. Ask questions and have had them answered to my satisfaction. I will stay in the pharmacy for at least 15 minutes after the injection and seek medical attention if needed. The eua is used when circumstances exist to justify the emergency use of drugs and. Except for the last two (2) questions, a “yes” response to any other question. Vaccine. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. (i) the patient and at least 18 years of age; I understand the benefits and risks of the vaccine(s). Vaccine administration record (var)—informed consent for vaccination section c i certify that. Please provide a copy of this form to your physician and/or healthcare provider for your permanent medical records. The eua is used when circumstances exist to justify the emergency use of drugs and. Except for the last two (2) questions, a “yes” response to any other question. I will stay in the pharmacy for at least 15 minutes after the injection and seek medical attention if needed. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. I consent to receiving/for my child to receive, the vaccine listed below. I hereby consent to the administration of the flu vaccine for which i have signed below be given to me or the person named above for whom i am authorized pursuant to sections 431.058,. I consent to receiving the seasonal influenza vaccine. Or (ii) the patient’s personal representative. In addition, i am aware that the personal health information. Except for the last two (2) questions, a “yes” response to any other question. Ask questions and have had them answered to my satisfaction. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. (a) the patient and at least 18 years of age; I consent to, or give consent for, the administration of the vaccine(s) marked. Vaccine administration record (var)—informed consent for vaccination section c i certify that i am: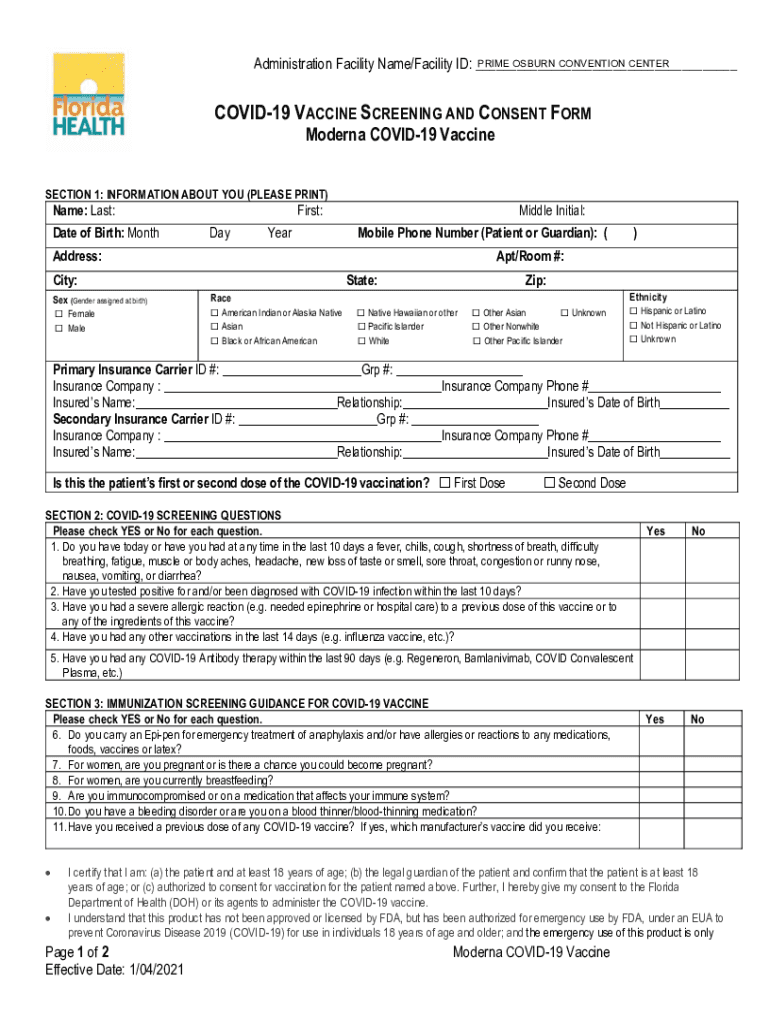
Moderna Vaccination Consent Form Fill Out and Sign Printable PDF
How to get vaccination consent from the public The JotForm Blog
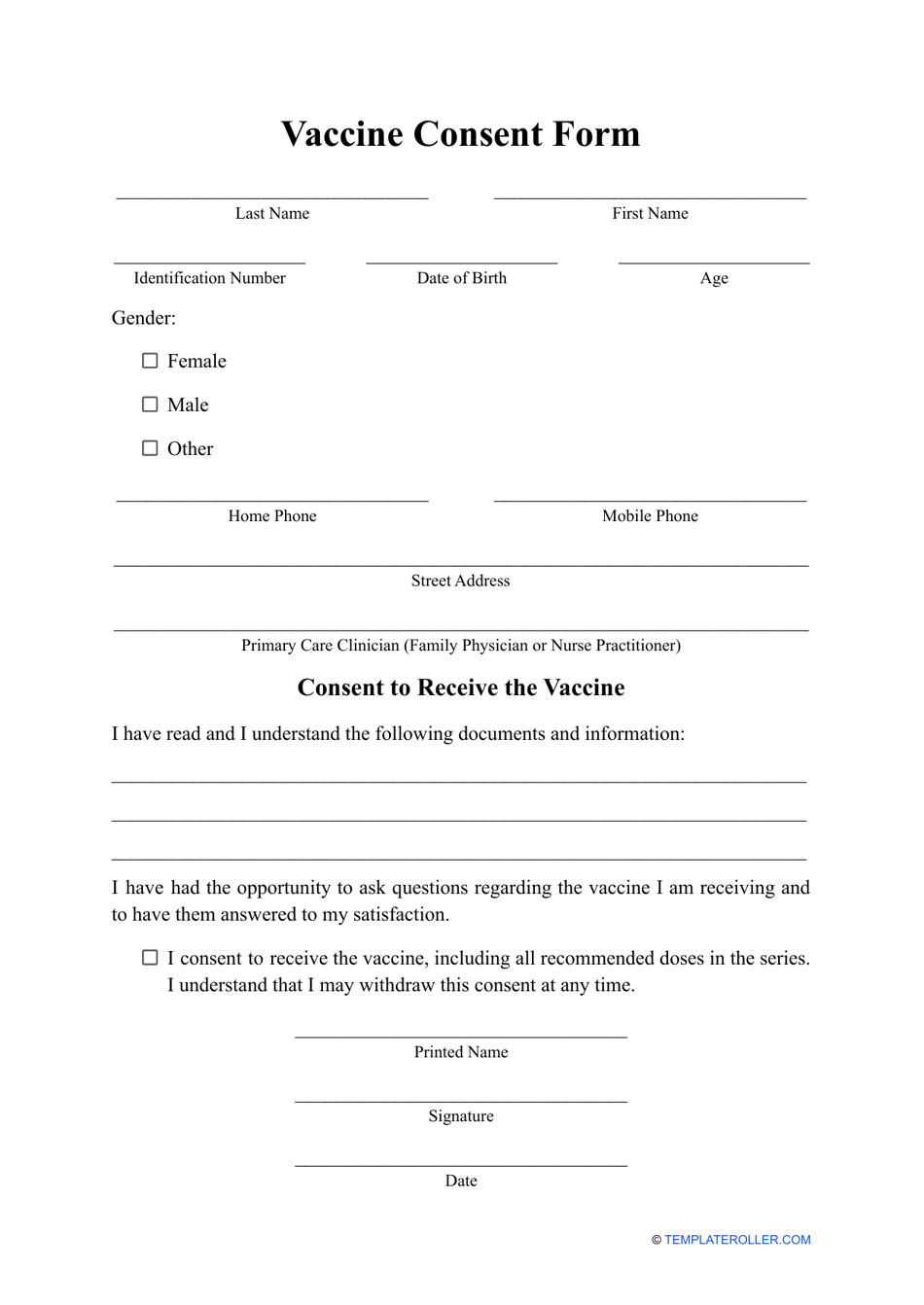
Vaccine Consent Form Fill Out, Sign Online and Download PDF
Blank Immunization Consent Form Fill Out and Sign Printable PDF

Vaccine Consent Form 2 Free Templates in PDF, Word, Excel Download
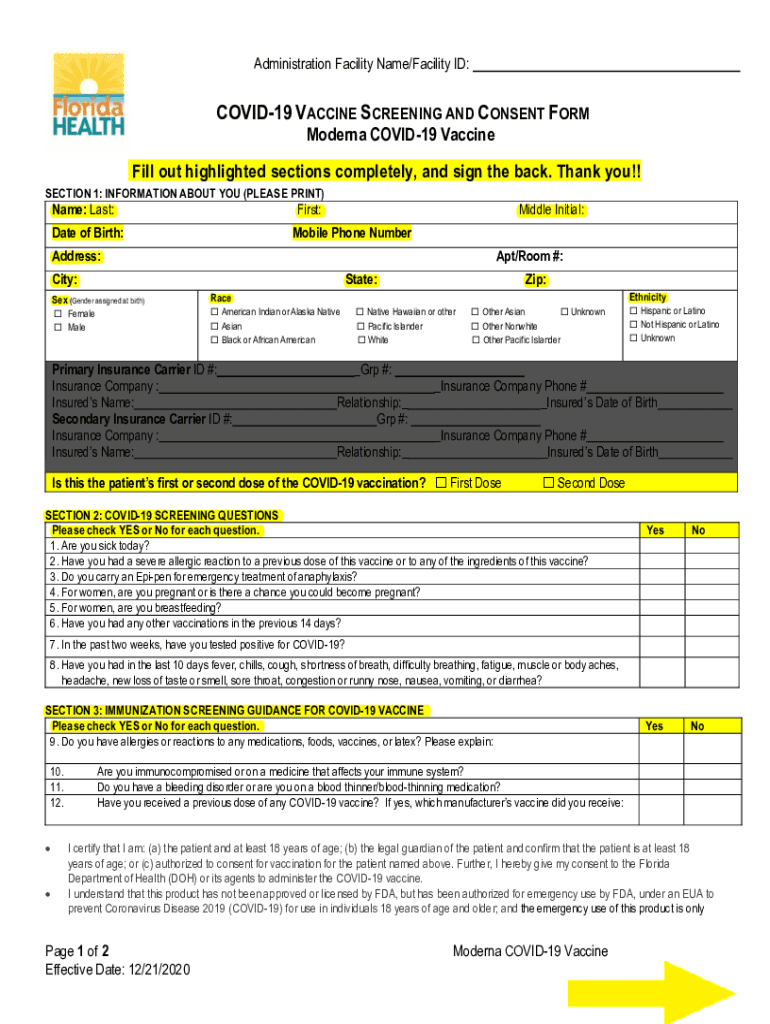
PDF COVID 19 VACCINE SCREENING and CONSENT FORM Florida Fill Out and
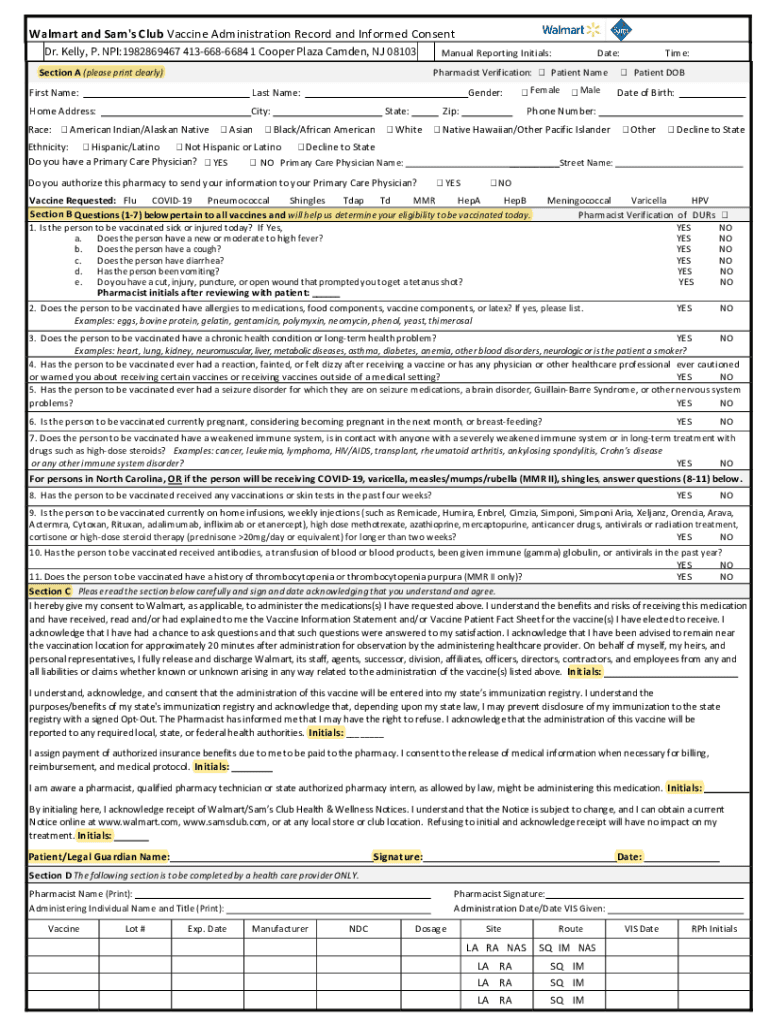
Walmart covid 19 vaccine questionnaire and consent form Fill out
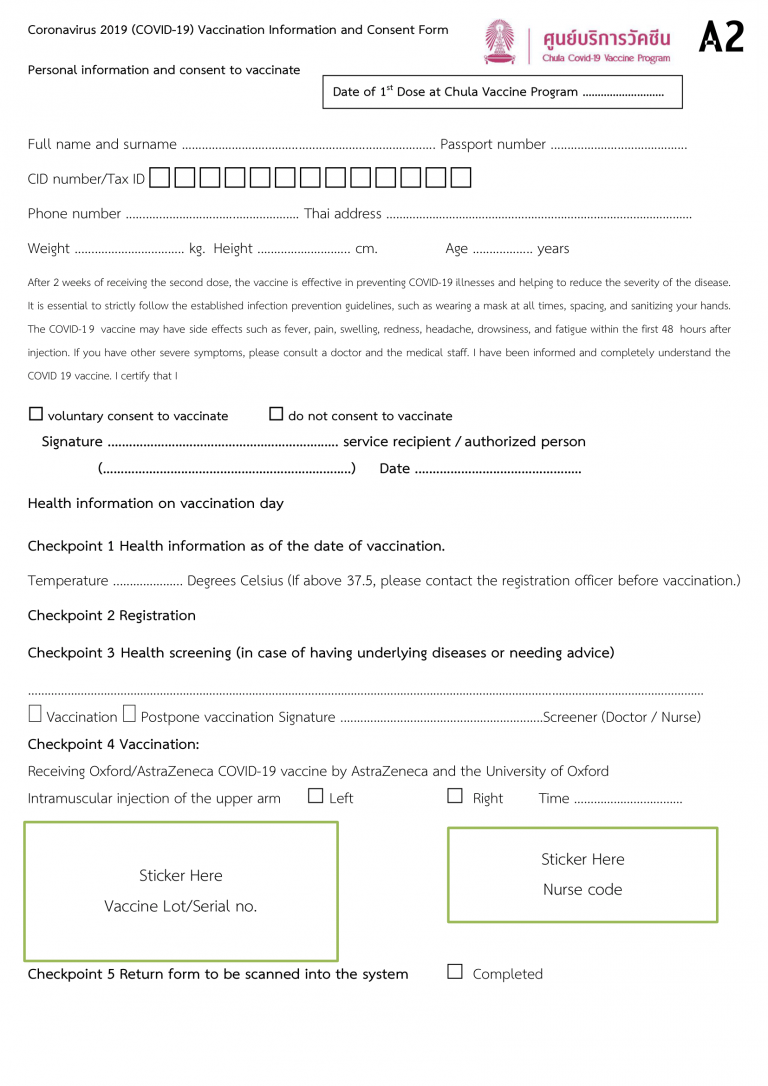
Consent Form and Vaccination Records Form for Coronavirus 2019 (COVID
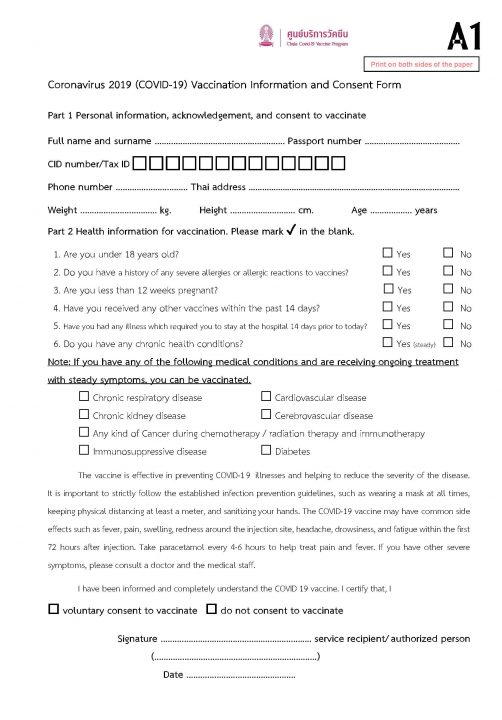
Consent Form and Vaccination Records Form for Coronavirus 2019 (COVID

Friendly Reminder Complete Your COVID19 Vaccine Intake Consent Form
Further, I Hereby Give My Consent To Walgreens Or Duane Reade And The Licensed Healthcare Professional Administering The Vaccine, As Applicable (Each An “Applicable Provider”), To.
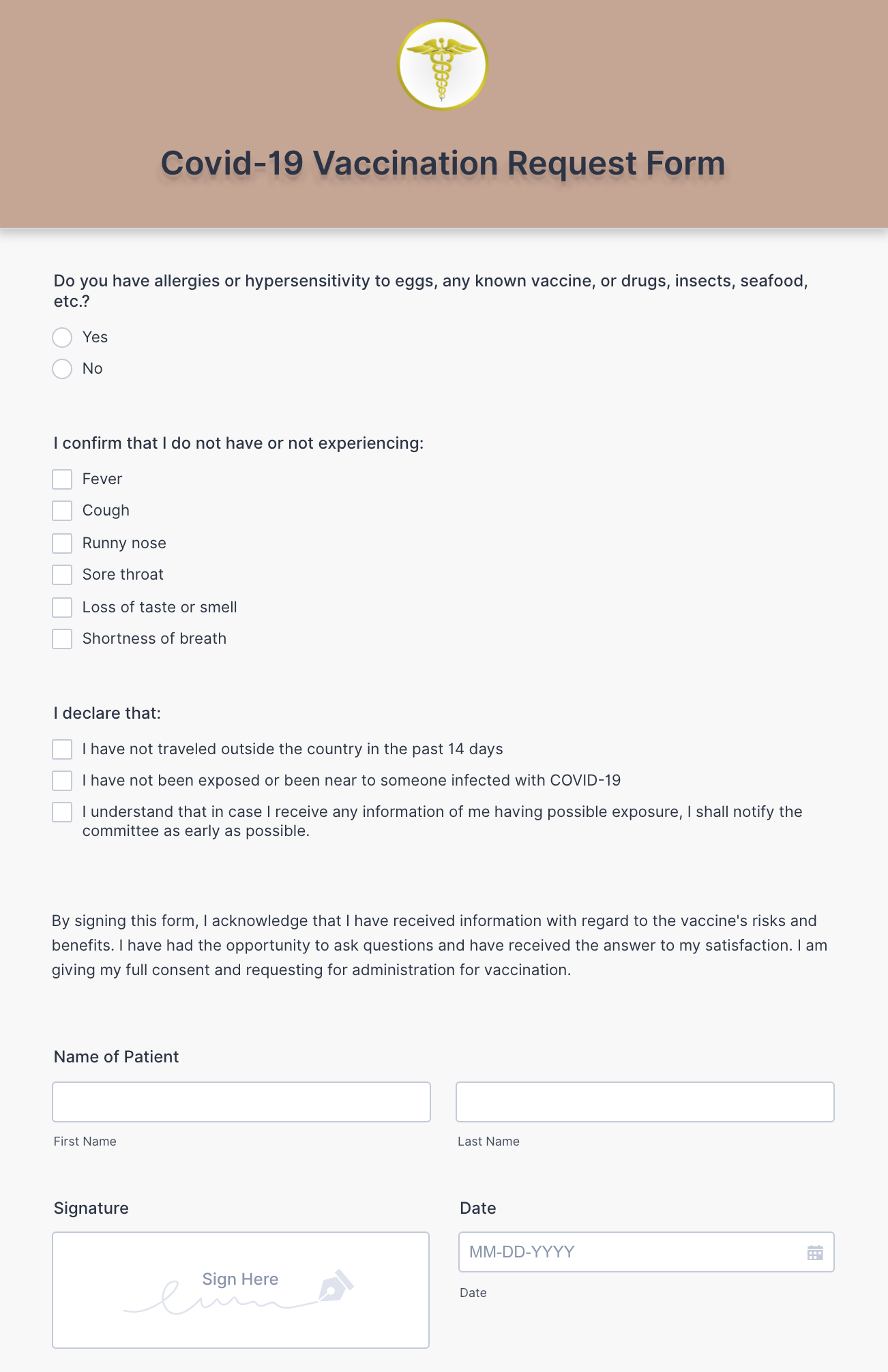
I Understand The Benefits And Risks Of The Vaccine(S).
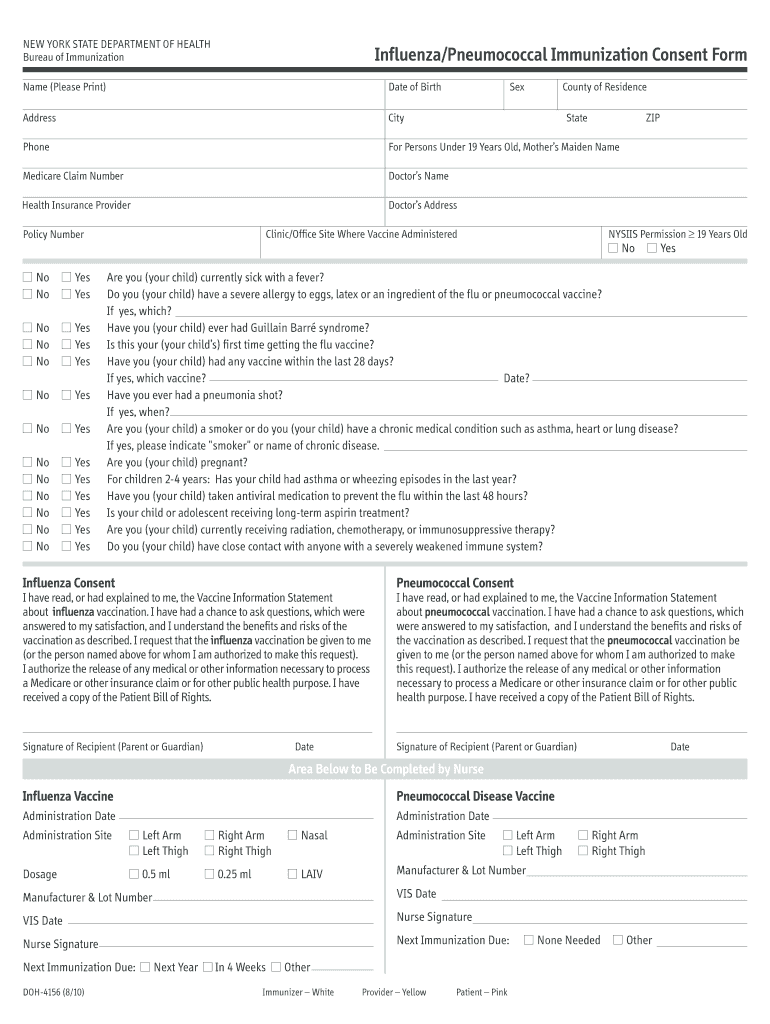
Tell Your Vaccination Provider About All Your Medical Conditions, Including If You Answer “Yes” To Any Question.
I Certify That I Am:
Related Post: